This is a very happy customer who used the quick straight orthodontic system …
Source: Testimonial Broad Street Dental Surgery – Orthodontics
Andrew Farr Dentist Broad Street Dental Surgery, Hereford

The Best Dental Implant Care in Hereford Dentist Andrew Farr at Broad Street Dental Surgery in Hereford
This is a very happy customer who used the quick straight orthodontic system …
Source: Testimonial Broad Street Dental Surgery – Orthodontics
Andrew Farr Dentist Broad Street Dental Surgery, Hereford
Andrew (GDC 115394) joined our team in October 2014. He was born and raised in Caerphilly, South Wales and at school he represented Wales through swimming. He studied dentistry at the University of…
Source: Andrew Farr
Mr A. presented complaining of his lower anterior teeth being misaligned. The LL2 was buccally placed and due to it’s position had caused previous trauma to the lower lip. He also complained that his lower anterior teeth were rotated as shown below.


Treatment was provided in the form of lower fixed short term orthodontics using the Quick Straight Teeth system. Minimal inter proximal reduction was required for LR3 to LL3 and the treatment was completed in roughly 6 months.
Retention was provided in the form of a fixed lingual retainer and Essix retainer. Composite build ups were offered to complete treatment however the patient was extremely happy and decided to leave this for now.
Andrew Farr

This is a nice little case that I wanted to share. It shows that sometimes the simple treatment plans and simple minimally invasive techniques can have a profound effect on a patient.
Mrs A. a 68 year old grandmother was concerned regarding the appearance of her central incisor, which her granddaughter had said looked “dirty.”
The UL1 (12) composite had leaking margins and a stained buccal enamel crack. The composite was removed and the enamel crack was cleaned with air abrasion. The UL1 (12) was then restored with A2 and enamel shade Synergy composite. The patient was very happy and so was her granddaughter!


Dentist Andrew Farr
Dental decay amongst five year old children is more prevalent in Herefordshire than any other county in the West Midlands. The Dental public Health Epidemiology Programme for England published in May 2016, show that 41.3% of five year old children in Herefordshire have had experience of or currently have dental decay. Compare that to our closest neighbours Worcester (27.3%) or Malvern Hills (17.7%) Shropshire (21.5%) then it is clear that Herefordshire is failing in the dental health of it’s children.
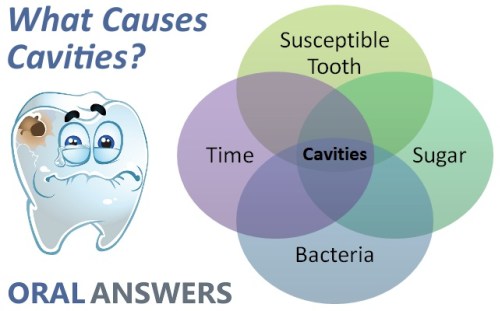
Tooth decay damages your teeth and leads to fillings or even extractions. Decay happens when sugar reacts with the bacteria in plaque. This forms the acids that attack the teeth and destroy the enamel. After this happens many times, the tooth enamel may break down, forming a hole or ‘cavity’ into the dentine.
Every time you eat or drink anything containing sugars, these acids attack the teeth and start to soften and dissolve the enamel. The attacks can last for an hour after eating or drinking, before the natural salts in your saliva cause the enamel to ‘remineralise’ and harden again. It’s not just sugars that are harmful: other types of carbohydrate foods and drinks react with plaque and form acids. (These are the ‘fermentable’ carbohydrates: for example ‘hidden sugars’ in processed food, natural sugars like those in fruit, and cooked starches.) Always check the ingredients.
Having sugary or acidic snacks and drinks between meals can increase the risk of decay, because your teeth come under constant attack and do not have time to recover. It is therefore important not to keep having sugary snacks or sipping sugary drinks throughout the day.
Children – at the age of 5 lack the manual dexterity to brush their teeth correctly and need supervised brushing. The Delivering Better Oral Health 2014 Toolkit recommends that all children between 3-6 years should brush using toothpaste containing more than 1,000ppm of fluoride. Children at a higher risk of developing decay should use a “pea size amount” of toothpaste containing between 1,350ppm – 1,450ppm fluoride.
Children at the age of 5 also lack the required funds to purchase sweets, fizzy drink, fruit shoot drink and other high products containing high levels of sugar. Parents therefore must take on the responsibility of caring for their child’s dental health with regular dental check – ups, good diet and good oral hygiene.

Bring your child as early as possible to visit the dentist. We need to reduce the incidence of decay amongst 5 year old children in Herefordshire to at least the level of our neighbours before we become the shame of the West Midlands.
Andrew Farr BDS(Hons) MJDF
This is just an experience that I would like to share. Whilst I was working for an emergency dental service over a weekend, a patient attended with a “swelling.” Little did he know but this swelling was extremely dangerous and required urgent attention!
The patient was not registered with a dentist, he had a fractured tooth in he lower jaw which had been painful a “few months ago” but had since settled. The swelling to the lower jaw had rapidly become worse over the past 48hours and now he was struggling to swallow.
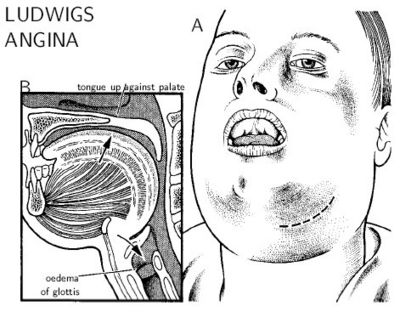
The patient had developed a diffuse dental abscess relating to the lower left molar tooth. This had spread down, under the jaw bone, had raised the floor of the mouth and was now crossing the midline over the patients throat and airway. He was developing a Ludwig’s Angina.
Immediately I contacted the on-call SHO for the local maxillo-facial department. The patient was immediately admitted to the maxillo-facial ward and ssurgical drainage of the abscess was provided. the patient had drains in place for a week and IV antibiotics.
This case shows the importance of regular dental check-ups and that any toothache/pain should not be ignored. By delaying dental treatment and ignoring the early signs of pulpitis/apical periodontitis the patient had placed himself at risk.
http://www.broadstreetdentalsurgery.com
Andrew Farr Dentist BDS(Hons), MJDF
(1) http://ludwigsangina.blogspot.co.uk/2011_12_01_archive.html
It is Diabetes Week from the 12th – 18th of June but what effect does it have for the dental team?
Diabetes (Diabetes Mellitus) is a metabolic disease where there is an imbalance of blood sugar due to either the pancreas not producing enough insulin or the cells of the body not responding properly to the insulin produced. This leads to high levels for glucose (sugar) in the blood. There are three main types of diabetes mellitus:
Type 1 diabetes is characterised by loss of the insulin-producing beta cells of the islets of Langerhans in the pancreas, leading to insulin deficiency which is needed for the absorption of glucose from the blood.
Type 2 begins with insulin resistance, a condition in which cells fail to respond to insulin properly. As the disease progresses a lack of insulin may also develop. The primary cause is excessive body weight and not enough exercise.
Gestational diabetes, is the third main form and occurs when pregnant women without a previous history of diabetes develop high blood-sugar levels
It is important to tell your dentist about your diagnosis. Whether you are type 1 or type 2 diabetic and if you are diet controlled, taking tablets or having insulin injections. This will allow your dentist to plan a preventative oral health programme, risk assess any oral health issues and also in the event of any medical emergencies – diagnose and treat accordingly.
 Diabetes and dentistry
Diabetes and dentistry
Although it may seem that diabetes and dentistry may have very little in common, studies show that Diabetes increases the prevalence of periodontitis, the extent of periodontitis (that is, number of affected teeth) and the severity of the disease. Patients with uncontrolled diabetes and established periodontitis may progress quicker and be harder to treat, compared with people who do not have diabetes. In well controlled diabetes with HbA1c of around 7% (53 mmol/mol) or lower, there appears to be little effect of diabetes on risk for periodontitis. However, the risk increases exponentially as glycaemic control deteriorates. Overall, the risk of periodontitis in patients with diabetes increases by 2-3 times.
Medication and effects?
It is important to tell your dentist what medications you are taking. Occasionally, medications can have other oral manifestations, such as lichenoid mucosal reactions (White patches) to metformin. Other oral consequences of diabetes may include xerostomia (Dry Mouth) resulting in increased risk of dental decay, thrush infections and chronic mouth ulcers.
It is important therefore that people who are newly diagnosed as being diabetic are also informed of the increased risk they have of developing periodontal disease. The Dental and Medical profession should encourage regular dental and periodontal assessments as studies have also shown that poor periodontal control can also have an negative effect on glycemic control.
With good glycemic control, good plaque control and regular/appropriate periodontal treatment, Periodontitis can be controlled and managed.
If you need a dentist or further advice please contact:
Andrew Farr BDS(H0ns) MJDF
The “new” surgery at Broad Street Dental Surgery Hereford is celebrating it’s first year anniversary since moving from it’s old premises (well a year and one month!)
We started with a shell of an office block on the top floor of the “Handelsbanken” building in Hereford. As the early pictures show we had quite a blank canvas to start with. The surgery would need to be designed to comply with many regulations including CQC, GDC, HTM 01-05 and IR(ME)R to ensure that the surgery was safe for our patients and operating to the highest levels.




With the help of Neil at Mercia Dental and Barry at Dental Style who helped with designing and fitting each surgery, the practice soon took on a better look and feel. A separate decontamination room was designed and fitted. The surgeries were fitted with ambidextrous Belmont chairs, new cabinetry and computers with views across Hereford and of the Cathedral.



We have also recently been Denplan Excel accredited and our patients can expect the best service and treatment in a new and modern setting, with a waiting room boasting the best views in Hereford.
We would like to thank the support of all the staff and patients during the move and development of Broad Street Dental Surgery and for their continued support.
At Broad Street Dental Surgery we pride ourselves on prevention, oral hygiene, diet advise and fluoride advise. Today was just like a normal day at the surgery until the very last patient of the day was half way out the door, then just out of the blue did the old Columbo “Just one more thing Mr Farr”
Mrs S. then produced a small bottle from her coat pocket – Eucalyptus oil blue gum for “teeth and gums” and a “healthy alternative to toothpaste” Mrs S. asked for my opinion and if it was better for her teeth than her normal fluoride containing toothpaste.
Being from a scientific (and quite sceptical) background where we are continuously and rightly reminded of evidence based dentistry I did just want to throw the product out of the window! With the level of decay that I see in children in the Primary setting I feel quite strongly about fluoride, topical fluoride and follow Delivering better oral health: an evidence-based toolkit for prevention
Fortunately for my ease on the back of the bottle in very small writing the bottle said “this product is not intended for the prevention and treatment of dental decay or gum disease.”
I explained what is fluoride and it’s benefits and risks.
Fluoride can greatly help dental health by strengthening the tooth enamel, making it more resistant to tooth decay. It also reduces the amount of acid that the bacteria on your teeth produce.
Children who have fluoride when their teeth are developing tend to have shallower grooves in their teeth, so plaque can be more easily removed. Plaque is a thin, sticky film of bacteria that constantly forms on your teeth.
The addition of fluoride to water has been researched for over 60 years, and water fluoridation has been proven to reduce decay by 40 to 60 percent.
Clearly the best form of decay prevention is good oral hygiene and diet. By reducing the amount of sugars/ refined carbohydrates in your diet which “feed” the cariogenic bacteria in your mouth and brushing with fluoride that helps to remineralise enamel and is in itself bactericidal.
Many reports have been published throughout the world about fluoride. After many years, the scientific conclusion is that fluoride toothpaste and correctly fluoridated water, salt and milk are of great benefit to dental health, help to reduce decay, and cause no harmful side effects to general health. Studies have not found any evidence that fluoride added to water causes harmful side effects.
People who are against fluoridation claim they have firm evidence that fluoride added to water is harmful. However, scientific analysis has not supported their claims.
Worldwide, over 300 million people drink fluoridated water supplies. Many millions more use fluoride toothpastes regularly. In the USA for example, well over half of the population have fluoridated water supplies. This has led to improved levels of dental health which in turn benefits general health.
Mrs S. was happy with our discussion. She was given information so that she could make an informed choice on her dental health. The Eucalyptus oil wasn’t thrown in the bin as such but Mrs S. will use it from time to time.
The battle against decay continues!
Mrs A. 32years old presented complaining of anterior crowding and really wanted to correct and align the upper central incisors.
Mrs A. had an Anterior open bite, excellent oral hygiene with no evidence of periodontal disease, caries or other pathology. She was happy to proceed with an upper fixed appliance only as she did not want or feel the need to correct the mild crowding in the lower arch. Mrs A. was aware that short term orthodontics would not correct the anterior open bite and this was not a concern for her.
Upper and lower impressions were taken and sent to Quick Straight Teeth (QST) for an upper fixed appliance. Pre-operative photographs and radiographs were taken.

By simply bonding the upper brackets and arch wire as instructed by QST and working through the arch wires supplied this case was completed without any IPR and within 5 months

Mrs A was fitted with both a palatal fixed retainer and given an Essix removable retainer. she was delighted with the final results. This case demonstrates how simple short term orthodontics can significantly improve aesthetics and maintain a very natural appearance.
Andrew Farr BDS, MJDF












